
What is aortoiliac occlusive disease?
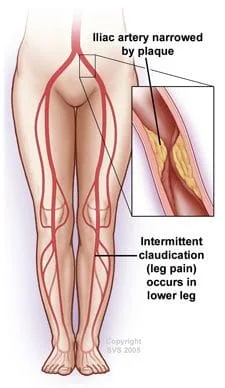
Your arteries are normally smooth and unobstructed on the inside, but as you age, a sticky substance called plaque can build up in the walls of your arteries. Plaque is made up of cholesterol, calcium, and fibrous tissue. As more plaque builds up, it causes your arteries to narrow and stiffen. This process is called atherosclerosis, or hardening of the arteries. Eventually, enough plaque builds up to interfere with blood flow in your iliac arteries or leg arteries. Physicians call this aortoiliac occlusive disease because it involves the aortoiliac arteries.
When your iliac arteries narrow or become blocked, your legs may not receive the blood and oxygen they need. This lack of oxygen is called ischemia and it can cause pain. In severe cases, sores or gangrene can develop, which can result in losing a limb. However, these developments are uncommon unless the process is not treated and is allowed to progress.
What are the symptoms?
Early in the disease, you may feel pain, cramping, or fatigue in your lower body when you walk or exercise. The pain with walking usually occurs in your buttocks, thighs, and legs. This symptom is called intermittent claudication because it stops when you rest. As the disease worsens, you may find that pain occurs when you walk for shorter distances. Ultimately, as the disease progresses, you may feel pain, usually in your toes or feet, even when you are resting.
Some men who have aortoiliac occlusive disease also experience erectile dysfunction, the inability to have or maintain an erection.
Aortoiliac disease may worsen if it is not treated. Signs that it has advanced include:
- Severe pain, coldness, and numbness in a limb
- Sores on your toes, heels, or lower legs
- Dry, scaly, cracked skin on your foot. Major cracks, or fissures, may become infected if left untreated
- Weakened muscles in your legs
- Gangrene (tissue death), which may require amputation
If you experience any of these advanced symptoms, it usually means that your leg arteries are blocked in more than one place. Your physician may need to treat more than one site to prevent gangrene or limb loss.
What causes aortoiliac occlusive disease?
- Atherosclerosis, or hardening of the arteries, causes most cases of aortoiliac occlusive disease.
-
Risk factors for hardening of the arteries include:
- Smoking
- High cholesterol levels in the blood
- High blood pressure
- Obesity
- Having a family history of heart disease
In rare cases, a condition known as Takayasu’s arteritis may cause blockages in your aorta and its branches. Takayasu’s arteritis usually affects young Asian women between the ages of 10 and 30. It is caused by inflammation in the arteries.
What tests will I need?
First your physician asks you questions about your general health, medical history, and symptoms. In addition, your physician conducts a physical exam. Together these are known as a patient history and exam. As part of your history and exam, your physician will ask you if you smoke or have high blood pressure. Your physician will also want to know when your symptoms occur and how often. A pulse examination that checks your pulse in several places in your legs for weak or absent pulses is part of your physical exam. For this test, your physician will simply place his or her fingers over pulse points.
After the history and exam, if your physician suspects you may have aortoiliac disease, he or she may perform tests to further define its extent and severity, such as:
 Ankle-brachial index (ABI)
Ankle-brachial index (ABI)
For the non-invasive ABI, your physician measures your blood pressure in your ankle and in your arm. Your physician will compare the two numbers to determine your ABI. Normally, the blood pressures in your ankle and arm should be about equal. But if your ankle pressure is half your arm pressure (or lower), your leg arteries are probably narrowed. To perform the ABI, your physician will use an ordinary blood pressure cuff and an ultrasound device. The ABI helps your physician diagnose aortoiliac disease, but it does not identify which specific arteries are blocked.
 Doppler ultrasound
Doppler ultrasound
Doppler ultrasound is another non-invasive test that uses high-frequency sound waves that bounce off of blood cells and blood vessels to show blood flow and problems with the structure of blood vessels. This test better identifies specific arteries that are blocked.
 Angiography
Angiography
There are three types of arteriography that may be performed: contrast arteriography, CT angiography (CTA), and MR Angiography (MRA). Contrast arteriography usually provides better resolution but is a more invasive test. Your physician injects a contrast dye into your arteries and then takes x-ray images. The structure of your arteries appears on the x-ray pictures because x-rays themselves cannot pass through the dye. This test finds the exact location and pattern of blockages. The dye is later passed from your body through your kidneys. If a blockage is identified and is appropriate for treatment by angioplasty and a stent, this procedure may be carried out at the same time. CTA and MRA are scans that are specifically dedicated to evaluating your blood vessels.
How is aortoiliac occlusive disease treated?
Lifestyle Changes
In mild to moderate cases, your physician may recommend that you change certain aspects of your lifestyle. If you are a smoker, the most important step you can take is to quit smoking. Chemicals in tobacco can damage your arteries. These chemicals can also increase your chance of having complications from aortoiliac occlusive disease.
In addition to quitting smoking, your physician may recommend that you maintain a healthy weight, follow a structured walking program at least 3 or 4 times a week, and eat a low-fat and high-fiber diet. These changes help slow hardening of the arteries. If necessary, your physician may prescribe medications to lower high cholesterol.
If you have high blood pressure, regular monitoring of your blood pressure and compliance in taking medication if prescribed is important. If you have diabetes, you need to control your blood sugar levels with diet and medication.
In addition, if you have diabetes, you may develop impaired sensation in your feet, a condition called neuropathy. Your physician may recommend that you receive foot care from a qualified healthcare professional and learn the basics of caring for your feet at home. This includes practicing foot hygiene, wearing protective, well fitting, and cushioned footwear, and avoiding injuries to your foot. This type of care can be very important because, as you lose the protective feeling in your feet, you can develop sores on them that may be difficult to heal.
Medications
If you do not have a disqualifying medical condition, such as heart failure, your physician may also prescribe cilostazol (Pletal), which may improve the distance you are able to walk without pain. Other drugs your physician may prescribe include aspirin or clopidogrel (Plavix), either of which can lower your chances of blood clots. Statins are a class of medications that your physician may use to control your cholesterol levels. None of these medications will "cure" you of the disease, but are important at relieving some of your symptoms, and may help protect your arteries from developing further disease.
Angioplasty or Surgery
If you have severe aortoiliac occlusive disease, particularly if it does not improve with the measures described above, your physician may recommend a minimally invasive treatment called angioplasty to improve the circulation in your legs. For more extensive blockages or those that cannot be treated with angioplasty, surgery to bypass or clear your blocked arteries may be required.
During an angioplasty procedure, which is sometimes performed at the same time as an angiogram, a long, thin, flexible tube, called a catheter, is inserted into a small puncture over an artery in your leg and is guided through your arteries to the blocked area. Once there, a special balloon attached to the catheter is inflated and deflated several times. The balloon pushes the plaque in your artery against your artery walls, widening the vessel. In some circumstances, a tiny mesh-metal tube called a stent may then be placed into the narrowed area of your artery to keep it open. The stent remains permanently in your artery. After successful angioplasty, blood flows more freely through your artery.


 Bypass surgery, usually done through abdominal or leg incisions depending upon the location of the blockage, creates a detour around the narrowed or blocked sections of your artery. A Y-shaped tube made of synthetic fabric, called a graft, is attached to your aorta above the blockage. The two branches of the graft are then attached to either your left and right iliac arteries or other major arteries in each leg (called the femoral arteries). Although more invasive, bypass surgery restores blood flow in about 85 percent of patients. Results are commonly maintained for 10 or more years.
Bypass surgery, usually done through abdominal or leg incisions depending upon the location of the blockage, creates a detour around the narrowed or blocked sections of your artery. A Y-shaped tube made of synthetic fabric, called a graft, is attached to your aorta above the blockage. The two branches of the graft are then attached to either your left and right iliac arteries or other major arteries in each leg (called the femoral arteries). Although more invasive, bypass surgery restores blood flow in about 85 percent of patients. Results are commonly maintained for 10 or more years.
An endarterectomy is a way for your surgeon to remove the plaque from your artery. To perform an endarterectomy, your vascular surgeon makes an incision in your leg or abdomen, depending upon the location of the blockage in the artery, and removes the plaque contained in the inner lining of the diseased artery. This leaves a wide-open artery and restores blood flow through your leg artery.
The best choice of the treatment depends upon the pattern of blockage as well as how much blockage you have. Your vascular surgeon will help you determine which method of treatment is best for your particular situation.
Revised September 24, 2009
|
|
Copyright by the NorthPoint Domain. See terms of use . |
|